by Craig Klugman, Ph.D.
Dale is a 45-year-old woman who lives in Southern California. She has been a patient of Kaiser- Permanente to treat her chronic illness, systemic lupus erythematosus (SLE). She takes hydroxychloroquine (brand name Plaquenil) which is the safest and most effective drug to control her disease. The drug helps control flare ups of her lupus, a situation that could cause serious illness and even death.
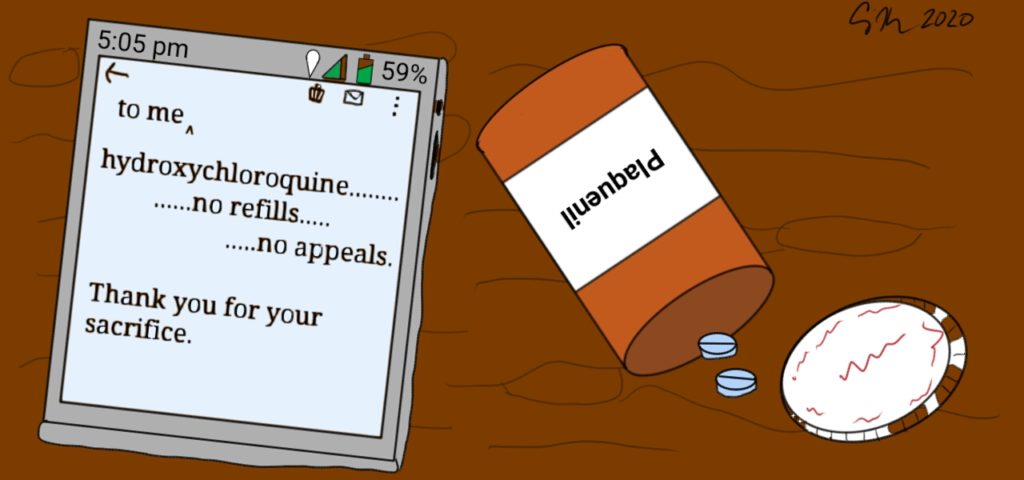
Dale provided Buzzfeednews with a copy of a message she received from Kaiser that informed her that her prescription would no longer be renewed. The message says that she should not contact her doctor for a refill, that even with a prescription they would not give a refill, and she should not request an exemption from this policy. The company is saving all of its hydroxychloroquine to treat “critically ill COVID-19” patients and people with acute lupus, but not chronic. The note offers “reassurance” in that they believe the drug will be in her system for 40 days and if she feels symptoms of her disease, she should talk to her doctor about alternative treatments.
 Dale takes her medication as prescribed. She takes a medication that has been approved for her condition by the FDA. Kaiser is saving its supply for experimental, off-label use. Why is it doing that? I do not know for sure, but can offer some ideas. Last week, during his daily news conference, President Trump claimed that chloroquine was a “game changer”, was FDA approved for this use, and would cure COVID-19. He offered no evidence. No part of his statement is true. The drug is being looked at in clinical trials. The drug is not FDA approved to treat COVID-19. But, his claim has led to a run on the drug and now there is an international shortage.
Dale takes her medication as prescribed. She takes a medication that has been approved for her condition by the FDA. Kaiser is saving its supply for experimental, off-label use. Why is it doing that? I do not know for sure, but can offer some ideas. Last week, during his daily news conference, President Trump claimed that chloroquine was a “game changer”, was FDA approved for this use, and would cure COVID-19. He offered no evidence. No part of his statement is true. The drug is being looked at in clinical trials. The drug is not FDA approved to treat COVID-19. But, his claim has led to a run on the drug and now there is an international shortage.
Evidence for effectiveness is sketchy. There are some limited case reports from China including a test on African green monkey kidney cells in vitro. That paper states that one effect of COVID is high cytokines and that in the petri dish, the anti-inflammatory effect of hydroxychloroquine decreased cytokine production: “We predict that the drug has a good potential to combat the disease. This possibility awaits confirmation by clinical trials. We need to point out, although HCQ is less toxic than CQ, prolonged and overdose usage can still cause poisoning.” The drug has potential, but needs to be studied. The studies are challenging because the drug can be dangerous.
Then there is an on-going study (no blinding, no random selection) in France. Twenty-six patients receive hydroxychloroquine and 16 served as a control. Within 6 days of the trial, six subjects in the intervention group were “lost” to ICU transfer (3), death (1), leaving the hospital (1), and side effects (1). Complicating analysis, six of the intervention patients also received azithromycin. On day 6, of those remaining in the experimental group, 70% were “virologically cured”. The authors state that their findings were so remarkable that they had to rush out the results, even though they are only reporting 7 days-worth of testing on a small group and their statistics do not include the 6 “lost” subjects nor the final outcomes of the patients.
Rather than wait for any of the 7 registered clinical trials (only 2 actively recruiting subjects) to go forward, President Trump announced this “game changer” and thus began a snake oil sale. Several people have already died trying to take this drug (or ones with similar names) on their own. Why do I suspect the cause of the problem is the presidential announcement and not everyone reading the studies? Because the French study combined drugs and no mention was made of azithromycin in his announcement. The FDA does not report a shortage of that antibiotic. The lesson is the importance of scientific literacy and good (appropriate) communication skills.
Thus, we return to Dale and her note from her health maintenance organization. As the Lt. Governor of Texas has suggested that the elderly should lay down their lives to COVID in order to get the economy rolling again, Kaiser has thanked Dale for sacrificing her health (and potentially life) to permit their off-label, experimental treatment whose effects are not totally known. Kaiser’s decision is nothing less than rationing of a now-scarce resource by removing an effective, approved, and life-saving drug from patients who need it, to hold it for hope and prayers. Kaiser was not transparent, did not have a stated method backed by reason as to how allocation decisions should be made, did not inform patients (and families) before acting, has no appeals process, and is practicing the opposite of evidence-based medicine—magical thinking.
In a crisis, the public is asked to make sacrifices. Twenty-one states (as of 11:59pm March 25) have asked or their populations to shelter-at-home. These orders cover 50% of the U.S. population. People have put off elective surgeries, dental appointments, and non-essential doctors’ visits. These are sacrifices but are not ones that threaten people’s health. Kaiser’s statement is akin to abandoning a patient. When firing a patient, a physician is supposed to inform the patient and offer a list of alternative providers to ensure continuity of care. Kaiser, as an HMO, is a one-stop shop (insurer, provider, and pharmacy) so there is no alternative. Even research subjects must be told risks, benefits, and alternatives; they can also leave the experiment at any time with no penalty. Dale can’t leave her insurer and provider until the next open enrollment period. She is held hostage. She was not a partner in her care and she did not consent.
For Dale, this is not a sacrifice for which she should be thanked, this is a notice that her chronic health condition is less important. That she is less important. What Dale is experiencing is a complaint that patients with disabilities world-wide often express, that they are treated as less than human.
As the COVID-19 pandemic worsens, a lack of personal protective equipment, hospital beds, ventilators, and health care providers will require that we make tough decisions. According to the 2012 Institute of Medicine Report on Crisis Standards of Care, triage decisions should be transparent, consistent, proportional, and accountable. Decisions and plans should also be evidence-based and constructed with community input. Kaiser missed the boat on all of these basic ethical principles. They also missed on how to communicate tough choices. Several organizations have produced guidelines and even scripts for how to have these tough scarcity talks. An electronic note is not how to have this conversation.
This story is a warning of how decisions on how to allocate scarce resources should not be made. Sacrifices will need to be made in this crisis, but they should be made in the light in line with strong ethical frameworks and values.